It has been brought to our attention that there is quite a bit of confusion surrounding CO 253, a Claim Adjustment Reason Code (CARC) that appears on the Remittance Advice (RA) when Medicare sequestration, a 2% reduction to the final amount, is applied to a Medicare Fee-for-Service (FFS) claim.
Often perceived as the CO 253 denial code because of its placement among all the other denial codes, CO 253 is improperly interpreted and managed by healthcare providers and their billing teams. We want to clarify any misperceptions you may have regarding CO 253 so that next time you see it on your RA, you know exactly what to do to maintain the financial stability of your practice.
Is CO 253 Denial Code Really a Denial?
No. CO 253, repeatedly referred to as the “Denial Code 253” or “CO 253 Denial Code”, is not a denial in a traditional sense. This is because Medicare is not denying you your right to reimbursement. Rather, it is reducing the amount by 2% because of sequestration, which we will explain in detail further in the blog.
So, technically speaking, CO 253 is not a claim denial. It is a payment adjustment that applies to all Medicare FFS claims because of federal regulations.
Then, Why Does 253 Have Group Code CO as a Prefix?
Claim adjustment reason codes are segregated into five group codes that help the provider identify why the payment was adjusted or denied. They are as follows:
- Contractual Obligation (CO) – the payment adjustment or denial was the result of a contractual agreement between the payer (insurer) and the payee (healthcare provider). Usually, when RAs are issued with this group code, the providers have to write off the adjustment, as they cannot bill the patient for the balance payment. Remember, 253 also falls under the CO group code.
- Patient Responsibility (PR) – The patient is responsible for the balance payment or the entire denied amount. For example, PR 27 is triggered due to coverage issues, or more specifically, when the healthcare service was performed after the patient’s insurance coverage was terminated.
- Payer Initiated Reduction (PI) – Indicates that the insurance payer initiated the reduction. Hence, the patient is not responsible for the balance payment.
- Corrections and/or Reversals (CR) – This group code is used when payment adjustments for previous claims are corrected or reversed.
- Other Adjustment (OA) – Any payment adjustments or denials that do not fit in the above four group codes are highlighted using OA.
Now that we know that CARCs are broadly divided into five groups, let’s try to answer the question.
Being categorized under the group code CO does not make 253 a denial code. As can be seen from our explanation of different group codes, CARCs briefly explain why the insurance payer adjusted the payment or why the reimbursement amount does not match the billed amount. The code can be a payment reduction, payment denial, or even payment correction/reversal.
In the case of CO 253, it is a payment reduction. So, let’s try to understand why the insurance payer, or Medicare specifically, reduces the reimbursement amount in the first place.
What is Sequestration in Medical Billing?
In the context of finance, sequestration means to take legal possession of someone’s assets. For example, when a debtor is unable to pay off his debt, the court orders the debtor’s assets to be sold off so that the creditor can collect his debt. However, in medical billing, sequestration denotes a 2% payment reduction on all Medicare FFS claims because of the Budget Control Act (BCA) of 2011.
In 2011, the U.S. government was facing the debt ceiling crisis, and the country was on the brink of default. To prevent this, Congress enacted the BCA, which raised the debt ceiling and introduced several measures for reducing government spending. One of these spending cuts was a lowered Medicare payout to healthcare providers. All payments made to Medicare providers after April 1, 2013, were reduced by 2%. This law will remain in effect until 2031.
Medicare notifies healthcare providers of this mandatory reduction with CO 253 or CARC 253. This payment reduction applies even to durable medical equipment (DME), orthotics, and prosthetics claims filed on or after April 1, 2013.
How is Sequestration Reduction Calculated?
The 2% reduction applies to the final amount. Medicare processes the claim, determines the approved amount, takes deductibles and coinsurance into account, and then reduces the reimbursement amount by 2%.
Let’s try to understand this with an example. Ready for some number crunching?
Suppose that a service was billed $1,000 as per the physician fee schedule (approved amount). Half of it, or $500, is the deductible (patient responsibility). Medicare will pay 80% of the balance $500, because the remaining 20% is coinsurance, which is also payable by the patient.
80% of $500 = $400
So, Medicare should pay the healthcare provider $400. However, when the 2% sequestration reduction is applied:
2% of $400 = $8
Then: $400 – $8 = $392
$392 is payable!
Therefore, the final reimbursement amount that Medicare will pay to the healthcare provider will be $392. CO 253 will appear on the RA alongside this payment adjustment.
Example of an ERA with CO 253
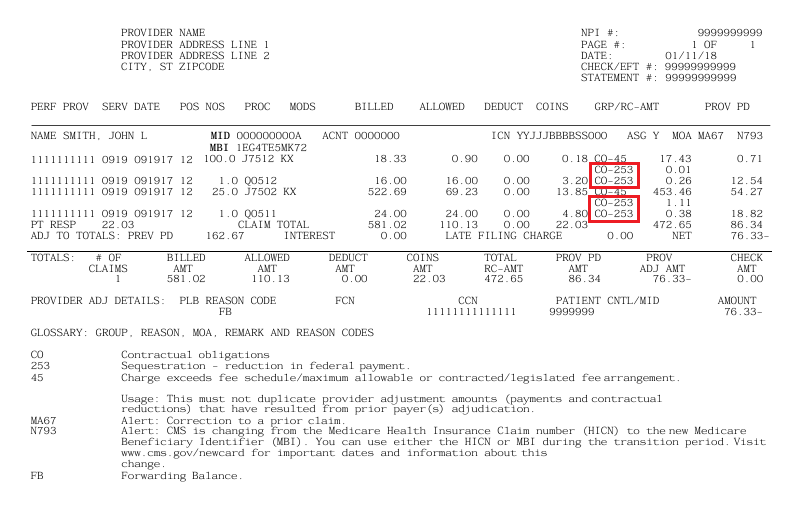
Source: CMS
In the above Electronic Remittance Advice (ERA), you can see that the total amount the provider billed to Medicare is $581.02. Medicare’s allowed amount for that service was $110.13. Out of which Medicare approved to pay $86.34. But after a 2% sequestration reduction and other adjustments, the provider received just $76.33.
Can You Appeal CO 253?
If it were a CO 253 denial code, you might have been able to appeal the payment denial and asked for its reversal after submission of relevant proof. Or you might have reworked the errors in the claim and resubmitted it for reimbursement collection. But, as we have discussed at length, CO 253 is not a denial in the real sense. It is a government-enforced 2% payment cut or mandatory adjustment that the providers must absorb and write off.
Please note that you cannot bill the patient for the balance after 2% Medicare sequestration is applied.
What Can You Do After Receiving CO 253?
For the ones adamant on using the term “CO 253 denial code”, this CARC is a hard denial. In other words, it is a non-negotiable payment reduction that the healthcare providers cannot fight and must accept as a contractual write-off.
So, if received, should you just let CO 253 erode your bottom line one claim at a time?
No. You must adopt the glass-half-full approach. Instead of focusing on the 2% loss, you should divert your efforts to the 98% gain and optimize other areas of your revenue cycle. For example, you must ensure that other billing errors like inaccurate coding, missing documentation, coverage issues, and payer or patient miscommunication do not lead to more denials and a significant loss in revenue. Implementing billing best practices will help you mitigate the impact of Medicare sequestration reductions.
If you need help with streamlined and efficient medical billing workflows, consider our medical billing services. We know how to optimize your practice’s revenue cycle and achieve a 98% clean claim rate.