In the United States, every 2 out of 3 adults have eye or vision problems. Still, a majority of them fail to get the necessary diagnoses and treatments. Why is this the case? Don’t Americans care about eye health? Well, it has more to do with affordability and complex health insurance rules than negligence on the patients’ part. According to the U.S. Centers for Disease Control and Prevention (CDC), more than 8 million adults know they need eyeglasses but cannot afford them.
Apart from outright denial of eye care coverage, there is another hurdle that patients and providers frequently encounter: Prior authorization for high-cost and specialized ophthalmology services, which often leads to delayed eye care.
In today’s guide, we will try to dissect the prior authorization process, rules, and challenges for ophthalmology services and procedures. But before that, let’s understand what prior authorization is and its significance in ophthalmology practices.
Prior Authorization in Ophthalmology Practices
Prior authorization, also known as pre-authorization, is an advance approval that healthcare providers obtain from the patient’s insurance payer. It allows the provider to confirm coverage for services and procedures that they intend to perform on the patient.
Typically, in ophthalmology, most routine services, like eye exams and screenings for eye diseases, are covered and do not require the payer’s pre-approval. However, costly services and surgical procedures should not be performed and billed to the payer without first obtaining a pre-authorization letter. This is because several ophthalmology services, like cataract surgery, are elective rather than medically necessary. And we all know the golden rule in medical insurance billing: only medically necessary services and procedures are covered and reimbursed.
So, in simple terms, prior authorization in ophthalmology practices is a safety net against claim denials. Providers can submit a request in advance to check whether or not the payer will cover the service.
Prior Authorization Process in Ophthalmology Practices
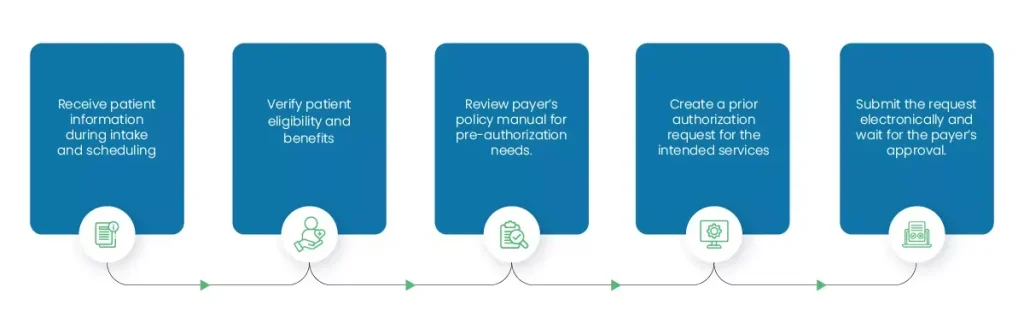
Ophthalmologists can get prior approvals for standard services within 3 business days. However, for complex and speciality services, it could take two to four weeks for a final decision. The good thing is that most payers process urgent prior authorization requests within 24 to 72 hours.
Prior Authorization Delays Faced by Ophthalmology Practices
Healthcare providers are generally required to obtain pre-authorizations for services and supplies, such as surgeries, pharmaceuticals, and durable medical equipment (DME). The field of ophthalmology is not exempt from these rules. The problem arises when the process of obtaining authorizations stretches to weeks and prevents providers from focusing on patient care.
The American Academy of Ophthalmology (AAO) states that physicians and their staff spend around two or more days each week negotiating with insurance carriers to secure approvals. This authorization challenge in ophthalmology delays patient care, leading to dissatisfaction and frustration.
Below, we have discussed some common reasons for prior authorization delays in ophthalmology practices. Take a look.
Complex Payer Requirements
Firstly, the rules and requirements for prior authorizations vary across payers. So, if Aetna wants you to obtain prior approval for an injectable inhibitor, Blue Cross Blue Shield may waive this step. Second, the criteria and format for submitting an authorization request are typically different for each payer.
But the last and hardest part? Prior authorization requirements for ophthalmology services are constantly updated. So, if earlier, you didn’t need pre-approval to perform laser surgery, it may now be a requirement, according to the payer’s updated policies.
All of the above factors complicate the process and delay prior authorization in ophthalmology.
High Volume of Requests
Did you know that in 2024 alone, around 53 million pre-authorization requests were submitted to Medicare Advantage insurers? That’s over 145,205 requests received per day! Just imagine. Payers must review each of these requests separately, often through the process of peer-to-peer reviews, to reach a decision and either approve or reject it. That’s a crazy volume of requests to process and finalize each day.
Due to this, the backlog keeps increasing, and what we experience are delays in ophthalmology prior authorizations.
Manual Workflows
Another major prior authorization challenge in ophthalmology practices is manual workflows. In an industry-wide survey conducted by JP Morgan, it was reported that 71% of providers still use paper and manual processes for medical billing, especially patient billing.
Manual and paper-based workflows are not only messy and prone to errors, but also time-consuming. The provider must first manually write a pre-authorization request, mail it to the payer, and then wait for days for a reply by mail. In contrast, electronic submissions (ePAs) are instant and can be reviewed the same day.
Frequent Documentation Errors
Ophthalmology practices that still use manual workflows, like typing the patient’s information during registration and front-desk verification, often end up with documentation errors.
Errors, like typos, spelling mistakes, and transposing numbers, are carried forward, conveying inaccurate information to the payer. This results in the prior authorization request being rejected. When this happens, the ophthalmology service remains unapproved until the provider fixes the errors and resubmits the request to the payer.
Ophthalmology Prior Authorization Changes
In 2025, America’s Health Insurance Plans (AHIP), Blue Cross Blue Shield Association (BCBSA), and several other leading health plans joined the U.S. Department of Health and Human Services (HHS) and Centers for Medicare and Medicaid Services (CMS) to announce multi-year initiatives to simplify and streamline prior authorizations.
Their proposed changes took effect on January 1, 2026, and were as follows:
- Reducing the number of services that require in-network pre-authorizations.
- Introducing a 90-day transition period for patients who switch insurance carriers during the treatment course.
- Making health plans responsible for clearly communicating prior authorization determinations, including support for appeals and other guidance.
- Requests denied based on clinical reasons will still be reviewed by medical professionals (peers).
Expected Changes in 2027
As for 2027, the following developments are anticipated in relation to pre-authorizations.
- Increased adoption of FHIR® APIs across all markets to accelerate real-time responses.
- Ensuring that 80% of prior authorization requests submitted electronically are processed and answered in real-time.
- Encouraging transparency through electronic pre-authorization submissions. (To date, half of the pre-authorization requests are submitted via fax or phone.)
- Development of standardized data and submission requirements to promote glitch-free, streamlined processes and faster turnarounds.
The goal for 2027 is to approve authorization requests at the point of care and ensure a faster and more consistent experience for healthcare providers.
Ophthalmology Services Requiring Prior Authorization
Prior authorization challenges in ophthalmology intensify when providers are unaware of the exact list of procedures and services that require pre-authorizations.
The table below gives an overview of the procedures and CPT codes for which ophthalmologists must obtain the payer’s prior approval.
| Procedure | Description | CPT/HCPCS Code |
|---|---|---|
| Cataract Surgery | Removal of the eye’s cloudy lens (cataract). May include replacing it with an artificial intraocular lens (IOL). | 66840, 66850, 66852, 66920, 66930, 66940, 66982, 66983, 66984, 66987, 66988, 66989, 66991. |
| Eyelid and Brow Surgery | Removing excess skin, fat, and muscle from eyelids and the brow area to correct sagging skin, drooping, and puffy bags. | 15820, 15821, 15822, 15823, 67900, 67901, 67902, 67903, 67904, 67906, 67908, 67914-67917, 67921-67924. |
| Glaucoma Surgery | Creating a tiny hole in the iris to improve fluid drainage and reduce eye pressure. | 0253T, 0449T, 0450T, 0474T, 0671T, 65820, 66150, 66155, 66160, 66170, 66172, 66174, 66175, 66179, 66180, 66183, 66184, 66185, 66989, 66991. |
| Refractive Surgery | Using lasers or surgical techniques to reshape the cornea or replace the eye’s lens to correct nearsightedness, farsightedness, and astigmatism. E.g., LASIK | 65767, 65771, 65772, 65775, 65785, 66985, 66999, S0800, S0810. |
| Intravitreal Anti-VEGF Injections | Medication is injected directly into the eye’s vitreous humor to block abnormal blood vessel growth and leakage. | C9399, J0177, J0178, J0179, J2503, J2777, J2778, J3590, Q5124, Q5128. |
| Corticosteroid Implants and Injections | Administration of potent anti-inflammatory medication directly to a specific site of inflammation, minimizing the side effects associated with systemic (oral) steroids. | J7311, J7312, J7313, J7314. |
| Ophthalmic Antibiotics | Antibiotics, including drops and ointments like moxifloxacin and erythromycin, are prescribed to treat bacterial eye infections such as conjunctivitis (pink eye). | J2280, J2281, J1364, J7099. |
Source: Versant Health
Common Reasons for Ophthalmology Prior Authorization Denials
The biggest prior authorization challenge in ophthalmology practices is request denial. What options are providers left with if the payer rejects the ophthalmologist’s request for a service’s pre-approval? Yes, they can speak to the patient, inform them of non-coverage, and communicate patient responsibility if they insist on the service/procedure, but this will delay patient care and stall the practice’s revenue cycle.
So, the easiest solution is to become familiar with the common denial reasons and prevent pre-authorization request rejections in the first place.
Pharmacy vs. Medical Problem
As we discussed before, ophthalmology prior authorizations are often denied when requests fall in the gray area between elective and medically necessary services. A similar issue arises when payers cannot clearly distinguish between a pharmaceutical and a purely medical service. This triggers delayed decision-making and denials because often, pharmacy benefits and medical benefits are billed separately.
This is especially true for ophthalmic treatments like intravitreal injections, where the pre-authorization process, request format, and payer portals are separate for pharmaceutical service pre-approvals and procedure pre-approvals.
High Frequency of Chronic Treatments
Ophthalmology treatments for chronic conditions like glaucoma and retinal diseases require monthly or bi-monthly interventions. This leads to prior authorization challenges in ophthalmology practices because a new request must be submitted for every single injection.
Instead of focusing on patient care, providers get stuck in a repetitive loop of paperwork for previously approved and medically necessary treatments.
Step Therapy Protocols
Another common reason for prior authorization request denials in ophthalmology is the “fail first” rule. According to this rule, providers must first treat patients with less expensive drugs and techniques and fail at them before moving to high-cost and specialized treatments. This is known as step therapy and helps justify the medical need for the intended procedure.
Without sufficient proof of step therapy, payers are likely to deny the pre-authorization request.
Complex Clinical Criteria
The criteria for ophthalmology prior authorization requests are quite complex. For example, in the application, the provider must mention visual acuity and Optical Coherence Tomography test results to explain the need for intervention. Even if a single data point is missing or the request is incorrectly formatted, it will trigger a denial.
Non-Speciality-Specific Peer Review
You might also be unaware that when ophthalmology prior authorizations are sent for review to the payer, there may not be a single ophthalmologist on the panel to perform the peer-to-peer review.
In simple words, insurance payers mostly employ general healthcare practitioners to review authorization requests. Due to the lack of specialty-specific knowledge and training, they may not fully grasp the urgency of a procedure or the benefits of a new FDA-approved drug, leading to unnecessary denials.
Streamline Ophthalmology Prior Authorizations with MediBillMD
Insurance payers view prior authorizations as a cost control measure, but for healthcare providers, this requirement is disruptive. In an American Medical Association (AMA) survey, 93% of physicians agreed that pre-authorization requirements result in care delays, and 82% reported that, due to delayed approvals, patients are forced to abandon recommended treatments.
Don’t let this be the case with your ophthalmology practice. At MediBillMD, we provide specialized ophthalmology billing services to tackle eligibility verification, pre-authorization, and claim generation issues for our clients. So, if you are encountering prior authorization challenges at your ophthalmology practice, count on us for expert assistance.